Foods that Kill Testosterone
We had Dr. Adam Nally, who is a family doctor and runs an obesity clinic, on the channel to talk about the Keto diet and testosterone. We had an excellent conversation.
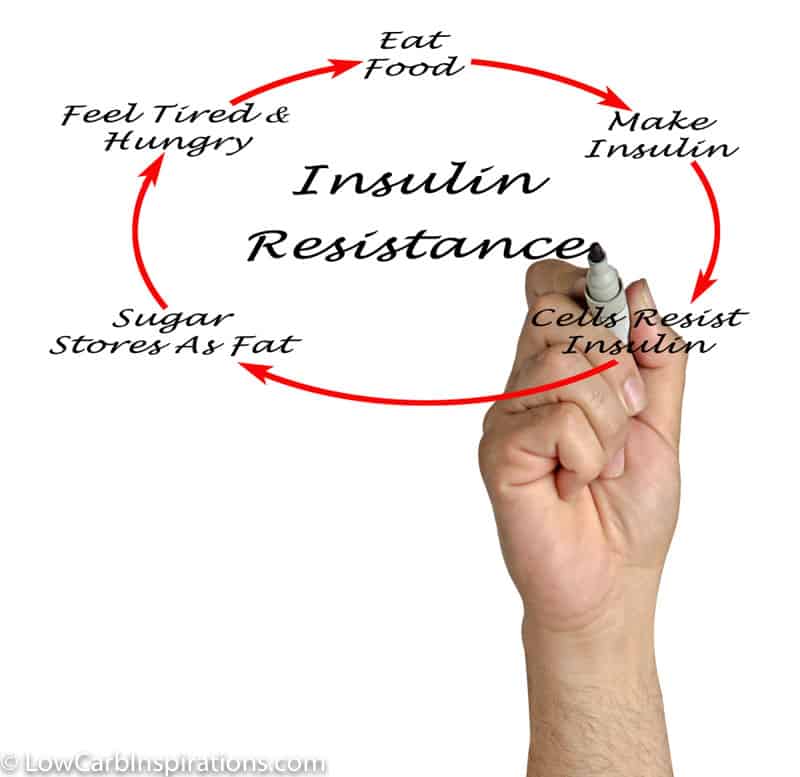
We have learned that the foods that kill testosterone are carbs and sugar! Most people can correct their testosterone or other hormone imbalances with the keto diet but it will take time.
If you enjoy watching Dr. Nally, be sure to watch the replay where he talks about Insulin Resistance and How to Start Keto video here.
I’ve transcribed the Facebook Live video on Testosterone and you can watch the replay here too:
Here’s the transcribed portion of this live broadcast:
Jennifer Marie: … welcome! So excited to have Dr. Adam Nally back on the channel. And tonight, we are going to talk about testosterone. I know the channel is mostly women, but believe it or not, we have a lot of people that, those women will go back to their men and definitely talk about testosterone. But it’s not just all about men, either. We are going to have some talk about women and testosterone, as well. Hey, Kathy Jerry Baker, how are you? Welcome.
Okay. So, before we get started, look what I got. My book came in, The Keto Cure. Ever since you were on, the last talk that we had about insulin resistance, I know a lot of people ordered the book. I ordered the book. And if you have the book and you’re following along, testosterone is Chapter 17 … or, I’m sorry, 14.
Dr. Adam Nally: 14.
Jennifer Marie: Chapter 14. Yay! So, hello, Gloria. Hello, Kristi. So, I’m excited. Are you excited? How have you been?
Dr. Adam Nally: Very well. Thank you for having me back. This is exciting to be here. You’ve got a great audience. And thank you for buying my book. I appreciate it.
Jennifer Marie: Yeah. You know what? After your talk about insulin resistance, I got so many messages-
Dr. Adam Nally: Oh, really?
Jennifer Marie: … that you really related to people, and you explained it in a way that was just so easy to understand. But I think the fact that you suffer from insulin resistance and you know the battle so well, I think that’s what makes you so relatable.
Dr. Adam Nally: Well, thank you.
Jennifer Marie: And I think just so many of us battle with insulin resistance, so it’s just a hot topic, too. But no, there were a lot of people that were really appreciative to that. And if you missed the replay, you can go back to lowcarbinspirations.com, and just search insulin resistance. And I have the replay, along with the transcribed video, there on the blog, and the link to his book. It’s a really good one. Let me just talk about the book real quick, if you don’t mind.
Dr. Adam Nally: Oh, yeah.
Jennifer Marie: Because I’m kind of excited about that, too. It’s titled The Keto Cure. And in the first half of the book, he talks about all these problems that we suffer from that keto can cure. So, he talks about the problem, he explains why it’s a problem, and then he goes on to say at the end of each chapter, what the Keto Cure is, and why it works. I mean, I love that. I love how it’s broken down, I love how it’s easy to read, I love that I can go … Well, the chapter that I’m on right now is 15, PCOS. So, I just love it.
Dr. Adam Nally: Thank you. For years, I started having all of these different diseases that were so responsive to a ketogenic diet. And there are 16 of them in the book. There are more, but those are the 16 that we had research on that we could actually have quantifiable evidence about, about using. But I have seen it affect others, as well. The cool thing is, we said, “Well, how can we make this understandable?” So first, we identified what is insulin resistance, as you talked about. And then, there’s a little tweaking with each of the different disease processes that you can use to treat that disease.
And so, a lot of people ask me, “Well, how do I treat my kidney stones?” or “How do I treat this?” And so, that’s really what we did, was we would try to give some basic information for somebody to have, some understanding as they walk into the doctor and say, “I have kidney stones, and I have insulin resistance. Can I apply these, and would these medicines benefit me, or can we change these medicines to work better?” And so, hopefully, that’s what it’s there for, and hopefully, that will give people some insight.
Jennifer Marie: Yeah. Kathy says, “yes, I bought the book.” Karen says, “Hi.” Hi, Karen. Heather says, “Is keto safe to do?” Heather, you are in the right place. Come back here every Sunday at seven, because we always talk about why keto is the right place, the right diet to do, the way of life. Yes, it is safe. We dive into lots of different things surrounding keto. Nicole Greene says, “My period is killing me. Was diagnosed with PMDD back in the 90s.” What is PMDD?
Dr. Adam Nally: Pre-menstrual dysphoric disorder. It’s actually a mild form of PCOS, is what it is. It relates heavily to the insulin levels and the testosterone levels. And we treat it often, like PCOS.
Jennifer Marie: Oh, good. So, tonight’s conversation will be really good.
Dr. Adam Nally: It will resonate with her.
Jennifer Marie: Yeah. So, I’m going to tell you guys, I am not at home. I am at my parents’ house, where you can see antiques in the background, and stuff. And the lighting is not that great. I’m out in the country in the middle of nowhere, so here’s to good Internet right now. If I’m fuzzy, that’s why. I’m doing my parents a favor and watching their house for two weeks, and taking care of chickens, and animals, and yada, yada, yada. Gail says, “Hello, Jen, Dr. Nally. Joining you from Mesa, Arizona.”
Dr. Adam Nally: Oh, Mesa, that’s cool.
Jennifer Marie: Yeah, that is. Patty said, “Hello, and thank you for your talk on insulin resistance.” See? So many people love that talk.
Dr. Adam Nally: Good, good.
Jennifer Marie: Nicole, “I’ve lost 17 pounds.” Way to go.
Dr. Adam Nally: Wow!
Jennifer Marie: Hey, Selma. Nice to see you on, Selma. Paula, from Canada. Let’s see, oh, we’ve got a lot of people. Hey, Sandy, Diana, Misty. Hey, Misty’s on! You know Misty.
Dr. Adam Nally: Mm-hmm (affirmative).
Jennifer Marie: Yeah. Nice to see you, Misty. She’s from AlternaSweets. She has the best barbecue sauce and the best ketchup on the planet.
Dr. Adam Nally: Yes, they have good food.
Jennifer Marie: Yeah.
Dr. Adam Nally: Good condiments for keto.
Jennifer Marie: Yes. Bonnie says, “Okay, we’re both very clear.” Okay, so let’s dive in.
Dr. Adam Nally: Well, let’s do it.
Jennifer Marie: Awesome.
Dr. Adam Nally: Awesome.
Jennifer Marie: Okay, so, do you want to start off with the problems, or do you just want to ask questions, or do you want the audience to ask questions? What do you want to do?
Dr. Adam Nally: Well, for those that don’t understand, and there may be some people. Let me give you some back story to what I see. We talk about insulin resistance, and one of the reasons … I guess I’m most passionate about insulin resistance is because literally, 85% of the people that walk through my doors have some degree of overproduction of insulin in response to starches and sugars. I don’t think it’s a disease, I think it’s a syndrome in response to the lifestyle and diet that we’ve been exposed to for the last 50 to 100 years.
And so, that’s one of the challenges. And so, we see this genetic response to high-carb diets and low fat, because we’ve been told to do that for the last 50 years. What’s happening is, this insulin level’s going up. And when the insulin level goes up, it starts to change the way bodies respond hormonally, and especially with the sex hormones. We see it with men and we see it with women. And not everyone will have the same exact response to that high insulin level because their body is designed to try to compensate and to try to maintain what is called homeostasis. And so, the biggest challenge that I see is that the insulin level starts to rise. And like we said before the last time we spoke, you’ll see a two- to 30 times greater insulin response to that piece of bread. So, if I eat a piece of bread, I’ve individually, produced 10 times the insulin response to that bread, and my body responds as if I literally, ate a whole loaf of bread. In some patients, it’s 30 times the normal value.
Well, what also happens is that the fat cells, as they become bigger and bigger, start overproducing hormones. And one of those hormones is leptin. Leptin gets overproduced, but because of the way fructose is handled, leptin can’t cross the blood-brain barrier. And adiponectin, which is the other hormone produced by fat, goes down, which turns down your cravings. So, leptin is supposed to signal, “Hey, I’m full,” and adiponectin is supposed to turn on the cravings. Well, neither of those signals are getting across the blood-brain barrier, and insulin’s going high.
And so, what ends up happening is, those two hormones change the way gonadotropin hormone is released, change the way luteinizing hormone is produced, in both men and women, through a pathway called CGRP. And I won’t go into all that. But basically what happens is, a high insulin and inappropriate leptin crossing the blood-brain barrier … leptin’s usually high, but it can’t cross. Both of these affect what’s called the HPG access. This is the hypothalamus, pituitary, gonadal access. So, there’s this set of hormones that is released when they’re supposed to be. You’re now damaging the way those are being released. And in men what happens is, the high LH starts to shift them from producing testosterone to overproducing estrogen and decreasing testosterone. So, you start seeing men … Most men should normally have a testosterone somewhere between 450 and 1100.
Because in the last 20 years, we have so many people with insulin resistance, a year-and-a-half ago, two years ago, the labs came out and said, “You know what? Looking at our data generally, in the last 10 years, we think our testosterone levels are now, too high.” So, they shifted the normal testosterone values down 250 points. So now, if you look at the reference range on the lab, normal male testosterone is 200 to 850. But I have men who actually have a testosterone of 300 who are symptomatic, but yet that’s still considered normal. So, if you have a doctor that doesn’t realize that value changed, your doctor’s going to say, “Oh, you’re fine. Nothing’s wrong with you,” yet that’s not true. Because what’s happened is, we now have a predominance of men who are under-producing testosterone because of an overproduction of insulin and poor leptin crossing the blood brain barrier.
And now, you have this group of men who is … they’re essentially, becoming eunuchs because they’re not producing testosterone. And you’ll start to see changes of high estrogen in these men. They’ll start to form, as my patients call them, man boobs, or breast tissue. They start to see testicular shrinkage. They gain weight around the belly. They get tired, they’re fatigued. Their libido’s gone. So, all these things start to happen with men.
Now, with women, the exact opposite happens. That luteinizing hormone is affected the same way, but what happens is, because men and women, the signal for testosterone and estrogen are different, they actually drop their production of estrogen and they increase their production of testosterone. Now, depending on how much leptin they produce, and women will do this differently, if your leptin signal passes through correctly, then you actually won’t produce the testosterone either. But if your leptin doesn’t cross, you will produce testosterone, and you’ll actually see varying levels of what’s called PCOS, or polycystic ovarian disease.
And there are four different stages or classes that you can read about in literature, and the OB’s go into this really heavily, but it all relates to how much fat you contain, how sick your fat cells are, how much insulin you’re producing, and how well that leptin crosses the blood brain barrier. And-
Jennifer Marie: I saw those four explained in chapter 16 in the book, too. It goes into detail.
Dr. Adam Nally: Yeah.
Jennifer Marie: Yeah, okay.
Dr. Adam Nally: So, there’s a lot of detail there. And hopefully, I’m not blowing past you with all these-
Jennifer Marie: No, no.
Dr. Adam Nally: … fancy hormone levels. But what’s important to understand is, when your insulin is high, as a male, your testosterone drops. When your insulin’s high as a female, your estrogen can drop can your testosterone can go up. You can form cysts on your ovaries, it decreases your libido as a female, and you have difficulty with conception, and fertilization, and those kind of things as well. So, we start to see menstrual irregularity, really heavy periods, or absent periods or skipping periods.
And so, insulin literally, flips the male and female hormone milieu in the patient. I see men that start to have increased female hormones, and I see women that start having increased male hormones. And that’s been common in my practice for 20 years. The amazing thing is that just shifting your diet, a ketogenic diet alone, fixes probably, 80%, just the diet alone.
Jennifer Marie: But it takes a long time.
Dr. Adam Nally: It takes about two years to get those hormones to balance out, correctly. So, you have to be persistent and patient with the diet. And you have to let those hormone levels downsize. And the big issue is that, because you have sick fat cells, those fat cells, until they start to shrink down, that hormone change doesn’t really happen. So, a lot of people come and get mad at me and say, “I’m not better yet, after two months.” It’s like, “Okay, but you still have fat cells that are not responding correctly. And as those fat cells shrink, as we help you return back to your normal weight you start to see that improve.” So, be patient with it, is the key.
Jennifer Marie: Yeah, be very patient. I’ve been doing these two-and-a-half years, and then I hit menopause, I think four, six months ago. So, I’ve been patient. I’m almost at the two-year mark. And then all these new symptoms, and it’s really frustrating.
Dr. Adam Nally: And menopause is a whole different ballgame. And again, you have to address it … It has its own nuances, which is actually exciting because when you get it right, you felt great. But if you haven’t got it right yet, you don’t feel so good.
Jennifer Marie: Yeah. Hey, Joe’s asking what the book name is. It’s called The Keto Cure. And we just dropped a link in the comments. Hey, Chris, could you pin that? If you could pin that link so people can find it. That’d be awesome. Yeah, and just so you know, half of the book is problems, symptoms, and fixes, and the other half is recipes. And I was going to tell you, are you working on any other books?
Dr. Adam Nally: Well, I have two … Yes, I have two outlines that I’ve been working on in my head. Once I get some substance to them, I’m going to present them to the publisher and we’ll go forward. But yes, they are there. I don’t know which one I’m going to present first. It really depends on which direction we go, but yes, we’re working on it.
Jennifer Marie: Nice. Well, if you need any keto recipes-
Dr. Adam Nally: Oh, yeah. Exactly.
Jennifer Marie: Yeah. I would be willing to help you and contribute if needed.
Dr. Adam Nally: Oh, I’m sure.
Jennifer Marie: For those who don’t know, let me just do a shout out real quick. My book, Keto Friendly Recipes Easy Keto For Busy People, is now number 7 in the whole-
Dr. Adam Nally: Yeah, you’re, last night you’re number seven. I looked on Amazon.
Jennifer Marie: Yeah, number 7 out of sales in the whole country. And, just so you know, Amazon dropped the price on the digital version to only 2.99. I don’t know how long that’s going to go for. I know it was 2.99 when I checked. It’s normally 12.99. That’s a $10 difference. So, I just have to tell you if you’re interested, you need a digital version, you want to get a copy for a friend, you’ve got to get it. Get it now while it’s cheap, you know?
Dr. Adam Nally: Cheap. Oh, yeah, no kidding.
Jennifer Marie: Yeah. Well, good. I’m glad to hear more books are in the works for you. That’s awesome.
Dr. Adam Nally: Yes.
Jennifer Marie: Good, good. Okay, back to … That’s a really good explanation of testosterone. So, fixing it, it’s going to take a long time. And depending on, I guess, how sick you are or how sick your fat cells are and how sick your hormones are, it could take a long time. It could even take longer if you’re sicker then, right?
Dr. Adam Nally: It can.
Jennifer Marie: So, what can you do to help … I mean, the diet, of course, is going to help you. But could you do anything better? Like, there are testosterone boosters out there, there are shots, there’s pellets, their creams, there’s all this other stuff. What could somebody do who has these symptoms of low testosterone? As a male, what can they do?
Dr. Adam Nally: Let me give you a little caveat that I learned the hard way. When I came out of school, we were trained if your testosterone’s low, treat the testosterone. For women, especially those … A predominant number of my patients are menopausal because there are over 65 and they’re in that stage of life. And so, we would treat their female hormones. But the challenge I found in the first few years of doing this was that they didn’t respond really well. And I could never figure out why. And then, what I realized was that when I started changing people’s diets, they responded really well. And then when we added on hormones where necessary, things just returned back to normal. And so, what I found is that if you attempt to treat the hormones before treating the diet and lowering the insulin, you will not be successful.
You have to bring the insulin down, you have to fix the leptin, you have to fix those hormones first. You also have to fix the thyroid first. And if those two things aren’t fixed, fixing the female and the male hormones really will not be effective, and you’ll essentially, be wasting those expensive hormones because people just don’t feel the way they should be feeling.
So, what I tell people first is, fix the insulin first with the diet. If you do have a thyroid issue, fix your thyroid issue. And then third, address the male and female hormones. And so, if you’ve got your thyroid under control and you’re following a good ketogenic diet, then what I find is that when you do add on testosterone as a male, or we add on estrogens, progesterones, and testosterones as a female, you feel fantastic. You feel so much better.
And I have a lot of people that are on hormones that, when we put them on a diet, those hormones need to be changed. They need to be adjusted up or down because suddenly, your body is now changing the way it’s handling those lives. And a lot of people will feel worse, but yet they never check those hormones. So, you’ve got to get those hormones checked. And then lastly, you want to check them regularly.
Jennifer Marie: Yeah. Okay, got it. So, you mentioned thyroid. How does somebody know if their thyroid is off? Because you said to do that, number two.
Dr. Adam Nally: I think we may have briefly mentioned thyroid last time we talked.
Jennifer Marie: We did. I think we did.
Dr. Adam Nally: A simple thyroid panel, the TSH and the thyroid panel, is for many people, adequate. However, I’ve started in the last five years, checking a reverse T3 and T3 levels, which is not part of the standard thyroid panel, because insulin affects them, as well. And so, if you’re not converting your T4, which is what the thyroid gland makes, to the T-3, which is what the rest of the cells below your neck need, act as the gas pedal for your metabolism, that may also make you feel sluggish. And that will actually affect your testosterone function and your estrogen function.
So, what I tell people is, get your TSH, get a thyroid panel, and get your reversed T3 check. And if those are normal, then we know, “Now, okay, now we can go on to the next step, which is your-” And I usually check all of this at one time, your male and female hormones.
Jennifer Marie: I am very vividly remembering that you did say this in the insulin resistant because I even put in the blog post on lowcarbinspirations.com, I said, “These are the ones that he specifically said to ask your doctor,” because not everybody will run those that you’re asking about. They just do the TSH, I think is pretty standard, right?
Dr. Adam Nally: Yeah, most doctors will just do TSH, because that’s what we were trained to check in school. But I find that you really, truly need the panel, you need the T3s, and you need the reverse T3s.
Jennifer Marie: Yeah. So, Kathy says, “Heard magnesium, zinc, and D3 is good for males with symptoms of low testosterone.”
Dr. Adam Nally: They’re good if you need them. The problem is that magnesium and zinc will inhibit each other, and so, if you take too much magnesium or too much zinc, you can block either of the receptors for either. D3 is only necessary if you are deficient, otherwise, you just make really expensive stool. And so, if your testosterone is low, using magnesium and zinc is important, but you won’t fix the low testosterone with magnesium, zinc, or D3. So, they help in stabilizing, but they won’t help fix the problem if the testosterone is low, either because of insulin or because you’re just not producing enough.
Jennifer Marie: Okay. Anne Winn Trout says, “Why do I keep getting yeast infections on the keto diet?”
Dr. Adam Nally: Remember that when you shift your pH … Well, let me back up. When you go on to a ketogenic diet, your pH in both your mouth, your gut, and your pelvic region will change. That pH changes. If for some reason, you have an underlying infection that needs to be treated, you may have that reoccurring. There are multiple reasons people have reoccurring infections. One is that they’re always moist or wet in that area, two is that they’re being inoculated because of sexual activity in that regard with someone who has a yeast infection that needs to be treated, three if you’re leaking urine… I have a lot of women who are at that age where they do have a little bit of leaking with coughing or sneezing, or they get a little urgency.
And if you’re leaking, funguses love moist, dark, wet places. And so, if you’re not staying dry down there, that’ll happen. Those are all reasons that create this environment that’s inhospitable or hospitable for bacteria or funguses that way. So, that’s something I would check with your doctor own because there’s probably an underlying cause there.
Jennifer Marie: Got it. So, Nancy says, “I have Hashimoto’s. I have nodules that we are watching. I’m on keto since mid-March. When should I test again?”
Dr. Adam Nally: Again, that’s something that you want to walk with your doctor through. The reason most people have nodules is because that’s part of the thyroid that’s trying to compensate for the part that’s not working. In my office with my patients, I’ll watch nodules every three to six months, depending on the type of nodule. And then, oftentimes, if you’re treating the thyroid correctly, those nodules will stabilize or shrink. So, that’s something to work directly with your doctor on. The issue is that the ketogenic diet dramatically helps the thyroid, but if you have genetic issues or various components that cause thyroiditis, you may always need to treat the thyroid with some thyroid component. Not always, but frequently, that can be the case.
Jennifer Marie: So, Carol says, “What do you do if you no longer have a thyroid?” Is that where you’re treating something if she doesn’t have it?
Dr. Adam Nally: Remember, again, your thyroid stimulating hormone, which comes out of the pituitary gland, tells the thyroid gland if you have one, to produce a hormone called T4. There are some other hormones that are produced, but T4 is the main hormone. We replace T4, which is basically a Synthroid or levothyroxine. That T4 hormone, when you take it orally if you don’t have a thyroid, is then converted into T3. However, if you’re still producing large amounts of insulin, insulin suppresses the deiodinase enzyme that converts the T4, that Synthroid, into T3 from your neck down.
And so, even though we’re giving you thyroid hormone, you’ll still be normal if everything is working right. But if you’re insulin resistant, that thyroid hormone may not be as effective. And so, that’s where it’s important to … that’s where I have patients who have insulin resistance, and they also have no toroid because they had the thyroid removed. We’ve got to watch the thyroid, too.
Jennifer Marie: Got it. So, Gloria Gross, she’s on here all the time. I love you, Gloria. She always asks the best questions, too. She said, “I had to ask my PCP for the T3, the T4, the reverse T3, along with the TSH. I take thyroid supplementation, and that lowers the TSH. Some doctors don’t seem to notice.”
Dr. Adam Nally: Well, remember, TSH is a signal from your brain trying to tell your body, “I need more,” or, “I need less.” TSH is really just a stimulating hormone from the pituitary gland, or pardon me, the hypothalamus, to the pituitary gland saying, “Hey, speed up or slow down.” Pardon me, it comes from the pituitary to the thyroid. We measure that hormone because that’s one way that we, as physicians, can determine, is the brain happy with the amount of T4 being produced. That’s really what the TSH tells us.
The T4 hormone is really, your foot on the gas pedal. And to be frank, T4 is converted into T3, and a lot of doctors don’t look at that conversion because we were never taught about that conversion. This is a new conversion that was just recently identified a few years ago. And our understanding of how the enzymes work in that conversion is really, really new. So, a lot of us were taught by endocrinologists to just, “Hey, just look at your TSH. That’s it. If the TSH is fine, it’s not a big deal.” But you really have to understand how that thyroid hormone is nuanced, and how insulin can play a role in the conversion of T4 to T3. And if your insulin is staying high, no matter how much thyroid hormone I give you, I may not make you feel better.
Jennifer Marie: That’s so interesting. What kind of, I guess, documentation or anything, could we give our doctor if they don’t know this?
Dr. Adam Nally: Well, the challenge is that the current literature, and even today, if you look it up in the most recent stuff that’s out there, that the predominant thought process for most endocrinologists is that, “You know what? For most people, if you’re watching TSH and a T3 and a T4, you’re probably fine.” But I have a lot of patients that come to me saying, “I still feel like my thyroid’s off,” but these are normal.
The challenge is that I don’t know of a good resource to give your doctor to say, “Hey, learn this or look at it.” But what you can ask your doctor is, say, “Can you look up reverse T3 and how that works? And can I have that lab tested so that I can determine it’s working or it’s not working?” A lot of functional medicine doctors, and a lot of … And I’m not a functional medicine doctor. I’m a general family doctor.
But there’s a lot of practitioners that are looking into age-related medicine. And we are finding that those docs in that area of schooling, we are starting to learn a lot more about thyroid. And so, that’s where those doctors will pick it up in that area. If you start to look at antiaging medicine, most of those physicians truly understand that process. And if your doctor doesn’t understand it, you could encourage your doctor to look at the antiaging approaches to treating thyroid.
Jennifer Marie: Got it. So, Linda says, “What’s the name of the book that’s on sale on Kindle for 2.99?” It’s the keto cookbook. It’s called Keto Friendly Recipes, Easy Keto For Busy People. And we put a link in the comments, also. Okay. So, as far as testosterone, then, I know we’ve had a couple of questions in our group, like are the boosters safe? Do you recommend those? Pills. I also want to talk about, once we do the diet and we have to kind of get off of those, how do you get off of those, as well?
Dr. Adam Nally: There are multiple approaches to treating hormones with testosterone. The challenge with testosterone as a hormone is, testosterone is destroyed if it passes through your stomach. So, if you’re taking an oral form of testosterone, it’s worthless. It’s not doing you any good. There are only two forms of testosterone that are effective, topicals, which are the creams, or an injectable. Injectables include pellets. Pellet is another way to use it. Pellets are great, too. The challenge with a pellet, though, is it stays there for four to six months, and you can’t change it. So you want to get your pellet dose correct.
The nice thing about topicals or injectables is, you can manipulate those doses. And once you find the dose that’s necessary, that if you decide you want to do a pellet, you can. In regards to estrogens and progesterones, there are synthetics and there are bioidenticals. I was trained to use synthetics, but what I found was, I could never get people balanced with synthetics. And the reason is that synthetic hormones, pharmaceutical companies, bless their hearts, cannot patent a real human hormone. So, if you have a real human progesterone or a real human estrogen, pharmaceutical companies cannot patent those. There’s a law that says you can’t patent them.
And so, if you can’t patent a drug, you can’t make money off a drug. So there’s no incentive to make an identical hormone to progesterone or estrogen. So, they make a derivative that works on the same receptor but is slightly different. The challenge is that all of these synthetic hormones, progesterones, estrogens, these all don’t cross the blood-brain barrier. And for women especially, and men, if your progesterone doesn’t cross your blood-brain barrier, you’re going to see insomnia, hair loss, confusion, cloudy-headedness, and general moodiness.
And so, for a lot of women who are using synthetic progesterone and estrogens, they’ll see these symptoms arise over time. We’ll balance out their cycle, we’ll fix that part, but they actually feel worse. And so, what I found is that using bioidenticals, a hormone that is identical to what your body usually makes, is really the most effective way because it will work on the top and the bottom of the body, works where it should, And you do well. The challenge is that a lot of the bioidenticals, you have to compound or have a compounding pharmacy make them for you. Because there’s only a couple of pharmaceutical forms that are bioidentical. And so, your doctor needs to be aware of how to find those and how to get them.
When you balance insulin and you get a ketogenic diet correct, then I recommend, look at your estrogen, look at your testosterone, look at your progesterone. I look at a couple of other hormones, pregnenolone, DHEA, and DHT, which help in expanding that component. But really, you want to look at those hormones and determine, are they in the range that you want them in. I shoot for mid- to upper-75th percentile range. When people’s hormones are in those ranges, they feel so much better. So, what we want to do is try to get a person in that range. Now, you may, just by changing your diet, hit that range normally. And a lot of people do, and so we don’t necessarily need to use hormones. But if we fixed your diet, and your thyroid’s balanced, and those hormones are still off, then we may want to consider supplementation.
Now, there are two schools of thought. With men, men should have normal testosterones, even in their 60s and 70s. But most men don’t, because of the way our diets influence that. The challenge, though, is as we age, there is a decline in those hormones generally, to some degree. And they will continue to decline until we pass away. The antiaging groups look and say, “Well, if we can extend those a little further, we may be able to give quality to people in their 60s, 70s, and 80s. And that’s what we do, and we see that benefit.
So really, it comes down to what you’re wanting to do. If you’re wanting to do some age reduction or antiaging treatments, then we want to look at, how do we use those hormones in a way that keeps you in a more normal range when you’re in your 40s and 50s. If you’re just saying, “Hey, I want to get off these pills,”, then I would say, “Okay, then we want to look at getting your insulin correct, getting your thyroid correct, and then just making sure your body lets those hormones return to a normal bracket for your age group.” So, there’s really two schools of thought in regards to what you’re wanting to do. And I work with patients in both arenas if that makes sense.
Jennifer Marie: Yeah. I know, I’ve been around a few males that have had their testosterone off. And man, let me tell you, those symptoms are real, and they are not to be played with. I mean, I’ve known complete gentlemen that turn really, really angry, and irritable at any little thing if your … I don’t, I think that if your testosterone’s too high. And then I’ve seen grown men cry like a damn baby if it’s too low. And they don’t cry. The symptoms are real, and the struggle is real. I want to read Scott’s comment here, real quick. He says, “I’ve lost 80 pounds, cured my diabetes and fatty liver.” Wow! Way to go, Scott!
Dr. Adam Nally: Good job, Scott.
Jennifer Marie: Yeah. He says, “My belly is all gone, but I can’t seem to rid the fat on my chest and my lats. Could this be hormonal?”
Dr. Adam Nally: Probably. Absolutely. More than likely, it is. And that’s where you want to check your thyroid, you want to get those male hormones to checked to see is … A lot of men that carried that much weight before may still be estrogen dominant. And so, that may be a male where we may need to adjust his progesterone with some testosterone to enhance that. We know that … I have a lot of males that lost 100, 150 pounds, and they never fully get back the testosterone levels they need. And if you can’t get that testosterone level back, you may see that abdominal or chest fat not fully improve until we get those levels back to where they ought to be.
And the thing about testosterone supplementation is that if you need it, it works wonderfully. If we overdo it, you will be rageful like the roid rage they call it with all the bodybuilders that totally misuse the steroids. If we under-dose you … And the challenge is, the body likes testosterone. And you can actually have some habit-forming addiction to testosterones, progesterones, and estrogens. You can actually [inaudible 00:33:11] the receptors. And all of the sudden we take away your testosterone when you’ve had it, you can, as a male, you all of the sudden become like a female going through her cycle, and tearful, and moody, and weepy.
And so, you’ll see those symptoms happen. And so, they are real. The goal is to understand number one, you have to realize that testosterone has a half-life of about seven days, and so, we have to dose it accordingly. Estrogen has a little shorter half-life, progesterone has a shorter half-life. And so, based on how long the medicine stays in your system and where we are shooting to get that range at, we want to give you a dose and a dosage form that’s going to be effective that way.
And so, that’s where different doctors will use pellets versus creams versus shots. And so, there’s a lot of nuance to that. And docs specialize in this, just because there’s so much nuance to it. But one needs to understand that it’s real, that a lot of times … The way I was trained, the way we were trained, we way overdosed testosterone way too much, and we had to learn to back it down. There are still doctors that I think, in my perspective, way overdose testosterone because they don’t understand how long it lasts, and that a small dose can be given more frequently and get more effective results in regards to testosterone, and then similarly, with progesterone and estrogen, as well.
Jennifer Marie: Yeah, I’ve heard of people going, not just once a week but twice a week, just to split that testosterone amount and not give it all at once, to kind of shock the body.
Dr. Adam Nally: Yeah, we don’t want to push your testosterone too high. But testosterone starts to fade, and it fades within a five- to a seven-day window. And so, we want to check that to see, where was your testosterone when we dosed it the first day, and where was your testosterone at day seven, and are we getting the peak and trough that we want to get out of it if it’s a shot. If it’s a pellet and stays consistent. If it’s a cream, it’s pretty consistent. We just need to get that cream higher or lower. And so, that’s really kind of the approach that’s made. But again, that’s something you want to work really closely with your doctor, and you want to have a doctor that understands how to do that. Some doctors, they claim they do well with it. But I went through some specialized training to understand how to do it because I was not taught how to do this at all in school.
Jennifer Marie: Yeah. So, we have a few more. Hey, Paula Jean. Nice to see you on. Hey, Pat Dyer. So, Michelle says, “What are your thoughts on iodine drops?”
Dr. Adam Nally: Iodine drops are important if you need them, but if you don’t need them, you can overdose. I’ve actually seen hypothyroidism and hyperthyroidism … Over-functioning and under-functioning thyroid occur because of someone overused iodine. Now, iodine, a lot of doctors pooh-pooh any iodine use at all. But I do have patients that need iodine, and so, if you need iodine, supplementing it is important. And if it needs to be supplemented, we want to supplement it in the appropriate range. But if you over-supplement iodine, you can actually stimulate abnormal thyroid function. So, just be careful with your iodine.
Jennifer Marie: Yeah. Isn’t there a test you can do, where you can rub iodine on you and look at it after 24 hours. And if it’s all absorbed, then you need it, and if it’s still there, then you don’t? Wasn’t that-
Dr. Adam Nally: That’s a naturopathic approach test, and I’m not familiar with the statistics and the validity of the test. I usually just do a simple blood test, and that gives me a good idea.
Jennifer Marie: Well, that’s another test to add for. If you’re going in, getting a T3, T4, reverse T3, TSH, you might as well ask for the iodine, too.
Dr. Adam Nally: Ask for the iodine, too, yeah.
Jennifer Marie: Let’s see, the lady that asked about yeast infections, Miss Trout, she says, “I’m insulin resistant. I check my sugars in the morning and it’s 154. After eating, it goes down to 120. I haven’t been able to get it down any further. Is it something to do with keto?” Well, keto will help lower that. But I would say what are you eating? Because eating a strict keto is going to really try and help not give those big boosts of those sugars. I don’t know, what do you think?
Dr. Adam Nally: If your fasting insulin is not going below 120, there’s either something in your diet, or the insulin resistance needs to be treated with either some supplements or medication to help that process. And remember, to get those numbers to start to get to be under 100 it may take some patients who are really insulin resistant, 18 months to get there. That’s the big key. And again, this is where just using your glucometer may not give you all the data you need.
You may need to have your insulin levels checked, you may need to see ketone levels, you may need to see those ratios a little more effectively. And this is where I literally, sit down with patients and I review their entire food journal for a week. And we’ll go through all these pieces because I’ll usually identify … They’ll tell me, “I drink five glasses of black tea every night.” And that tea plays a big role with insulin, and causes the Somogyi effect to kick in, and has some other things that can happen. So, I’ll usually go through a really intense diet journal review with them, because that’s the challenge with the Internet is, there is no way to know for sure what may be causing that. Other than the fact that we know it’s abnormal and we know there’s insulin resistance there, and so that’s where a close look at your actual diet, all of your medical history, what medicines you’re using, is really helpful.
Jennifer Marie: When you mentioned supplements for insulin resistance, is that something like metformin, or what would that be?
Dr. Adam Nally: Well, there are some really good studies that came out using berberine, especially with PCOS. Berberine is the active ingredient in turmeric. And when we isolate it out and we use … 400 to 500 milligrams three times a day of berberine was actually shown to perform equivalently to 500 milligrams of metformin in patients with PCOS. But it doesn’t have diarrhea and the stomach, or the G.I. upset that you get with metformin. In fact, it outperformed Metformin and weight loss. And so, berberine is actually a really effective supplement that I use for patients that aren’t actually diabetic. They haven’t hit the diabetic range, but they have insulin resistance, and those blood sugars are not fully responding. We can use berberine and see some real nice improvement and enhancement of the handling of insulin and blood sugar as that person is healing.
Jennifer Marie: Is there anything wrong if you take the berberine and you don’t need it? Will it make you feel weird? I ask, because I think-
Dr. Adam Nally: It can, yes.
Jennifer Marie: … that happened to me.
Dr. Adam Nally: And this is interesting, because Peter Defty, who’s an endurance athlete and endurance coach in California, they did some studies with Jeff Volek and Steve Finney … they’re 100 and 150 mile runners, so these ultra-marathoners. And they actually looked at some comparison, in regards to what happens with the body with exercise versus the use of berberine or metformin … actually, it was metformin. They didn’t actually use the berberine. But because berberine and works along similar mechanisms of action, there may be a similar effect with berberine.
What we found is that metformin, if you’re not exercising, metformin is a fantastic medicine. But during that window of exercise, if you use metformin, it actually suppresses what’s called the VO2 max, or your ability to burn fat at a higher level during that window. So, these ultra-marathoners actually saw worsening performance if they used metformin during the time of their exercise. So, it actually does play a role in its inhibition of the mitochondria.
And so, this is … We are really getting into the weeds with this, in regards to the pharmacology, and this may be way above your audience. But what I tell patients is, if you’re physically active and you’re exercising regularly, and I’m talking about weightlifting, notable yoga, walking, running, to where you’re breaking a sweat, you probably don’t want to use your berberine during that period of time. And I would talk to your doctor about whether to use metformin during that period of time or not.
But if you’re not exercising really heavily, or you’re diabetic, that’s where metformin comes into play. And berberine also plays a role there. But I actually started using berberine outside the window of exercise, because exercise actually enhances the use of blood sugars even more efficiently than the metformin or the berberine, at least according to that study. And so, that’s something that’s still new information we’re still trying to understand. But it’s pretty powerful, in regards to really pushing the window on healing, if that makes sense.
Jennifer Marie: That is so interesting. Joanne Jacqui says, “Wow, it’s wonderful to listen to somebody who knows what he’s talking about.”
Dr. Adam Nally: Thank you.
Jennifer Marie: She wants to know, “Do you have an MD twin in the Boston area, by chance?”
Dr. Adam Nally: I wish I did. I don’t, I don’t. I would love to have a license all around the country, and be able to go everywhere and help all these people, but that’s too difficult to do.
Jennifer Marie: Yes, yes. So, Tara says, “Maybe this was answered. Would you treat PCOS?”
Dr. Adam Nally: Absolutely. A ketogenic diet is the only effective treatment to PCOS that I have found in 20 years.
Jennifer Marie: That’s awesome. That’s awesome. Okay. So, Lisa says, “I’ve had my gall bladder-“
Dr. Adam Nally: In fact, let me add a caveat. If a person comes into my office with PCOS, I will warn them, “I’m going to put you on a ketogenic diet. But if you’re not careful, you’ll be pregnant in two months.” Because I’ve had multiple women who come in, who’ve never been able to get pregnant. And I put them on a ketogenic diet, and they’re pregnant in two months. And they’ve failed fertility clinics and all sorts of things. So, I will warn you, a ketogenic diet can cause pregnancy. So, be aware of that.
Jennifer Marie: Yes. No, that is a real thing. Because in our group, the Low Carb Inspirations Plus Keto Friendly Recipes, we have a group of 183,000 people, and it’s a thing. It’s been talked about.
Dr. Adam Nally: It’s a real thing, so if you have PCOS and you’re not used to having to use protection, you will become fertile real fast. I’ll just warn you of that.
Jennifer Marie: Isn’t that amazing, that just a change in a diet, in only two short months can be that powerful? Just think about that for a moment. I mean, that’s what gets me excited, is that this, we call it a diet, but it’s a way of life. It can be delicious, it doesn’t have to be diet restrictive, it’s good food. You just got to tweak it a little to make it work for you.
Dr. Adam Nally: Yep.
Jennifer Marie: So I get so excited about that.
Dr. Adam Nally: It makes your pants fall off, and it can also get you pregnant. So just be careful of that.
Jennifer Marie: That’s correct. Okay, so Lisa says, “I’ve had my gallbladder removed, and I have trouble digesting fat. Is there anything that I can do and take over he counter that may work better than ox bile? Does she need a digestive enzyme?
Dr. Adam Nally: She may need a digestive enzyme. And there are some that you can get over the counter. There are some that your doctor can prescribe for you. I would probably consider using, and there may also be … Oftentimes, people who have had their gallbladder removed also have some significant reflux issues and a change in their bacterial flora. So, looking at an appropriate probiotic, looking at the use of apple cider vinegar or treating reflux is also an issue, and then using … Unfortunately, ox bile or the bile components are the only biliary forms that I found that you can add. But sometimes using a pancreatic enzyme replacement for a month to two months is also helpful. Again, there are over-the-counter versions and there are prescriptive versions. If the over-the-counter measures don’t seem to be effective, then I would talk to your doctor about that.
Jennifer Marie: Got it. Debbie’s asking … I’m so behind on comments, guys. Debbie says, “Is testosterone good for Diabetes 2?”
Dr. Adam Nally: So, there’s an interesting study, and these were not ketogenic patients. But there’s actually two studies that actually demonstrate that men who had low testosterone, if they were given testosterone to an adequate level to treat their hypogonadism or their low testosterone, it actually enhanced their ability to control their blood sugar and enhanced their ability to lose weight.
So, we know that supplementation does play a big role in speeding the process of healing. And so, I use it, I guess, aggressively that way to try to push the whole process along. It will heal on its own if you give it time, but again, I come from a perspective of better living through chemistry if you can use it correctly. So, if we can enhance or speed the process along by maintaining normal hormonal levels by a small amount of supplementation, then I’m all for that. And I find great success with that. And that’s what the literature shows, as well.
Jennifer Marie: So, Gloria says, “I’ve heard a supplement that’s made by standard process called cholecol, C-H-O-L-E-C-O-L, she’s not sure of the spelling, would be helpful. It’s a bile salt.
Dr. Adam Nally: I’m not familiar with that particular one, but I know that there are a number of bile salts out there that are similar to ox bile. Again, that may or may not be beneficial. That would be something you’d have to check. I don’t know that supplement, specifically.
Jennifer Marie: Got it. Jenny Manning says, “Type 2 diabetic, keto six months, off all meds.” Wow!
Dr. Adam Nally: Congratulations.
Jennifer Marie: Right?
Dr. Adam Nally: Yeah.
Jennifer Marie: Her A1c is 5.6, but blood sugar stays around 130, 140. Also on thyroid meds.
Dr. Adam Nally: Again, the sugars are running high, and part of that is related to the size of the fat cells. And again, that’s where we start looking to see, would a supplement be beneficial, would a short-term … I have patients that come to me saying, “Doc, I feel great. I’m losing weight. I’m going to stop all my blood sugar medicines.” And I say, “Okay, well, hold on just a second. Let’s back up for a minute. Some of these medicines are going to help you in the process, and some of them, we want to stop.”
And so, a lot of people want to cold turkey their pills, and I get that. But again, we also want to look to see, will any of these help you in the process of healing With that ketogenic lifestyle? And that was one of the reasons I wrote the book, was that with each of those disease processes, which medicines or supplements will be helpful for you? And that’s really what those 16 different diseases we address in there are all about, saying, “In this process of using a ketogenic diet, we could use this, this, or this to speed the process.”
Jennifer Marie: Yeah. So, Scott came back with another question. He said, “Are there any over-the-counter testosterone supplements that are at all effective?” Didn’t you say if it’s over the counter and you’re putting it orally, it’s-
Dr. Adam Nally: Yeah, the stomach acid has a pH of one, and it literally destroys testosterone when it hits the stomach. Nobody’s been able to perfect an oral testosterone. And all those over-the-counter … You’ll notice that all the over-the-counter testosterone supplements are advertised after 11 o’clock at night. That should tell you something about that supplement.
Jennifer Marie: Yeah, exactly. So, Sherry Hall Toole says, “My husband is prescribed .7 ml every 14 days. Would it be better to take .35 ml every seven days?”
Dr. Adam Nally: I personally, find that dosing testosterone every seven days is more effective, and people feel better, because the supplemented testosterone is gone out of your system within seven days. And so, that second week often, the person’s testosterone is gone. And in order to get that testosterone to stay high enough in those last seven days, you have to overdose testosterone for the first seven days. So, I find that people are more likely to need estrogen blockers if we are overdosing the testosterone that way. And so, I find that dosing every seven days in my practice seems to be the most effective way to do it.
Jennifer Marie: And I even know people who go twice a week, just to not get that boost.
Dr. Adam Nally: Not to get that boost so high, yeah.
Jennifer Marie: Yeah. Let’s see, Sherry says, “That’s testosterone injectors I give him.” Yeah.
Dr. Adam Nally: Yeah.
Jennifer Marie: “Such great info. Thank you both,” Paula Jean says. So, Brenda says, “We were told in the past that women should not take estrogen because it can cause an increase in breast cancer. Is that a myth?”
Dr. Adam Nally: Let’s clarify that. There was the giant Women’s International Health Study that was done, and what support and to understand in that study was that they looked at nurses. Many of these were retired nurses, or women over the age of 60 to 65 that were placed on estrogen and did not need estrogen. So, they had normal estrogen levels, and they didn’t need it. So, I never recommend using estrogen that way.
The second issue was that they noticed an increase in breast cancer in this group at the end of the study, but when they actually went back … And initially, it was blamed on the use of the estrogen. But when they actually went back and looked, those cancers were there prior to the study starting, as a primary component of that. Second is that most of those cancers, many breast cancers, are estrogen- or progesterone-positive, meaning if I give you estrogen and you have a cancer that’s estrogen-positive, it’s going to grow faster.
So, it’s important to understand that if you have a breast cancer, and it’s estrogen- or progesterone-receptor positive, it’s a problem giving you estrogen or progesterone, and you need to work with your doctor very closely about whether or not that is something you should consider or not. However, what we know is that just giving you estrogen does not cause breast cancer. If there is a cancer present already, it will make it grow faster. But there’s no causative effect.
What we know causes breast cancer is an abnormal ratio of progesterone to estrogen. So, if you are estrogen-dominant or you are progesterone-deficient, you are more likely to have a breast cancer form. So, the ratio of progesterone to estrogen is really the key. We want that estrogen to progesterone ratio to be balanced. And what we know is that many women, as they go into menopause, that balance is thrown way off. And so, what I focus on heavily in my practice is not so much trying to give them more estrogen, it’s trying to balance that ratio and get that ratio back to a normal level where we know that when that level’s normal, they’re much less likely to have cancers form.
Jennifer Marie: That’s so interesting. So, Pat says, “My glucose isn’t terribly high, but after 10 months, I still have too much hunger to fast successfully.” She’s wondering if the berberine may help. “Maybe my insulin is still too high.” So, would you suggest berberine as a supplement, maybe, for somebody?
Dr. Adam Nally: Well, berberine is a great supplement for someone who’s insulin resistant or has an impaired fasting glucose. When you’re not in that diabetic range, I find that berberine is really effective in that regard. But the issue is, if a person’s having trouble fasting, there’s still something in that diet that’s stimulating an insulin response. And so, we need to look really closely at what’s driving … At your last meal, you had something that’s really pushing that insulin up, and you need to identify what that is, because that high insulin will cause you to have tremendous cravings as you pass through that period of fasting.
Jennifer Marie: We talked about this last time. There was a cure that’s monk fruit, that’s approved keto, but in 50% of people, you mentioned in the last slide we did that some people who are insulin resistant, there’s about half of those that are triggered by monk fruit.
Dr. Adam Nally: Yes, I’m one of those that’s triggered by monk fruit. My insulin goes up if I eat monk fruit. My blood sugar won’t, but my insulin will. There are a number of the keto-approved pastas that actually do that to me and to a number of my patients.
Jennifer Marie: Really?
Dr. Adam Nally: Oh, yeah. So, I don’t know if I told you, we went to the Keto Con big show that was there where I met you at, and there were 500 exhibitors there. And they all had great tasting food, but as I went through and looked at the ingredients on most of those, only three of them, I could have. Otherwise, the ingredients in a lot of those products, for someone like me who’s really insulin resistant, just totally throws me off. [crosstalk 00:52:55] And I can’t use them.
Jennifer Marie: There was starch in some.
Dr. Adam Nally: Some of them had starch, and some of them had sweeteners that cause a problem. And so, that’s a big issue. I have a lot of people that, I think we talked about it last time, leaf-based teas, your green tea, your black tea, your oolong teas, those will spike insulin. So, you have to be careful with those. So, there’s a lot of things that will throw you out of ketosis if you’re not careful. That’s the whole reason for writing the book, is, “What are all those things that I can fine tune that may be playing a role there?”
Jennifer Marie: Yeah. So, Gloria says, “My granddaughter and her husband adopted two children. She went on the keto diet, and now they have their own baby.” That just goes-
Dr. Adam Nally: Yep. I warned you ahead of time.
Jennifer Marie: Yep. And Faye says the same thing. “My nephew and his wife are pregnant after 20 years. Keto on.” See?
Dr. Adam Nally: Wow.
Jennifer Marie: That’s so funny. Okay, so Vicki says, “I’ve been diagnosed with lipidema, a fat disease.
Dr. Adam Nally: Lipidema. It’s an abnormal deposition of fat, often on the hips and the legs, that’s out of proportion to the rest of the body.
Jennifer Marie: Okay. So, she’s been on keto for two years and lost 80 pounds, but have, and then the sentence cut off. So, let’s see, did she come back? I don’t think she finished that. She says she carries all of her weight, just like you said. Okay, I don’t know what the question is. Put your question back in there, because it cut off. Okay, so Krista says, “When will my BIH pellets start working? It’s going on week five.” Doesn’t that takes six weeks?
Dr. Adam Nally: Well, if they’re pellets, she should be feeling them immediately. And if she’s not feeling them, then the question is, is there a thyroid issue, is she still notably insulin resistant and it’s not letting her feel the effect of those pellets, or are the pellets just maybe too, the dose may be wrong? So, that’s where if you’re at week five and you don’t feel like they’re working, I’d be chatting with your doc, and checking your diet, and checking your thyroid.
Jennifer Marie: Yeah. They probably missed the thyroid. Kristi Wilkins Ruelle says, “April of 2018, A1c was at 14. Went on keto two months later. A1c in September 2018 was 5.8.”
Dr. Adam Nally: Congratulations.
Jennifer Marie: “I will never-” she says, “I will never quit keto.”
Dr. Adam Nally: That’s awesome.
Jennifer Marie: Way to go.
Dr. Adam Nally: That’s awesome.
Jennifer Marie: Okay, Scott says, “I took my A1c from 10.4 to 4.6 in five months.” That’s amazing.
Dr. Adam Nally: That’s amazing. I see that all the time, but it still amazes me.
Jennifer Marie: I know.
Dr. Adam Nally: Because there are not drugs, there are not combination drugs that do that. In fact, I have patients on insulin with A1c’s of 11 that never get their A1c below seven, and yet you just change the diet and wham! It’s amazing.
Jennifer Marie: Wow. Okay, so Linda says, “I’m reading this book right now. I have advanced Crohn’s. List colon and part small intestine. Struggling with weight as the foods that make me feel better are high carbs. Just had a severe flare, and had to take steroids for three weeks. Back on keto this week. Gained 17 pounds. So frustrating.”
Dr. Adam Nally: So, the challenge is that, for those with Crohn’s disease or inflammatory bowel disease, it’s a vicious cycle. And the foods that in the short-term make them feel good are the comfort foods, the carb foods. But it’s the high carb and the high insulin response that, two or three weeks after that, make the Crohn’s flareup. So, what I tell patients is, with Crohn’s and inflammatory bowel is, the statistics show that if you will follow a ketogenic diet, there’s a 65% reduction in Crohn’s and inflammatory bowel flareups.
In fact, I have two patients right now that are in the practice that are completely off all of their inflammatory bowel drugs because of keto. And so, they’re doing fantastic. A lot of people think they have to cycle. If they flare up, they can’t do keto. That’s not true. You can do keto. And even on the prednisone, you can do keto. The cravings for carbs will be there, but they can still do keto in that period of time. And what they have to look at is not just the short-term feel, but the long-term effect.
Jennifer Marie: So, when they still have the cravings, I’m not a big supporter of BHB on an everyday use, but I am wondering in that situation, where they have the cravings, would you recommend some of the BHB salts, just to help them, as like a crutch?
Dr. Adam Nally: Yeah, because it’ll give them fuel, number one. It’s a liquid form and they’ll absorb it more effectively. They’ll get immediate fuel from it. And it has an anti-inflammatory effect to it. And so, the beta hydroxybutyrate, or the ketones in a liquid form in that case, are great. Again, being cautious with the type of sweetener that’s in those ketones is going to be a big factor. So, you want to make sure you’re being careful, because not all ketones are created equal. But that’s a perfect disease process, for looking at using exogenous ketones in place of some shake or a meal. And that’s how I use it with a lot of my patients.
Jennifer Marie: Got it. Well, we have to wrap up. We’ve already been here-
Dr. Adam Nally: Wow.
Jennifer Marie: … an hour. And I’m sorry, I didn’t get through all the questions. Let’s take one more, because Krista asks, “So, how do you test your insulin level?”
Dr. Adam Nally: How do I test mine? I test mine with an exogenous, with a Keto-Mojo, or a Precision Xtra blood … I use blood. The breath test fluctuates so much, and they’re so different between patients that I have trouble giving people good advice. Although, it does give you a number, that number varies for everybody. So, I just use blood for most people, and for myself.
Jennifer Marie: Yeah. I do too. So, Krista, if you’re part of the Low Carb Inspirations Plus Keto Friendly Recipes Facebook group, go in there. And in the welcome, we have a bunch of discount codes for a lot of products that will help you. And one of them … We have two different types of blood meters that we recommend. So, I think that’ll help.
So, I know we talked a little bit about you coming on again. I think the subject may be some sort of hormone, maybe estrogen dominance or something. Because I know that we’ve got a lot of ladies who would maybe, love to talk a little bit more about that. So, we’ll work our schedules.
Dr. Adam Nally: Love to.
Jennifer Marie: I’ve got Dr. Boz coming back.
Dr. Adam Nally: Cool.
Jennifer Marie: Yeah, she’s coming back next Sunday. So, we’ll be able to catch up with her and her trip to China, and whatnot. So, she’ll be on. But I’ll talk to you and see if we can’t get you back on a week after. We’ve got to coordinate our schedules. So, we’ll do that. Thanks for tuning in, everybody. This has been an excellent conversation. I really enjoyed it. I hope all of you got some really good information about testosterone, and berberine, and what test to ask for, and hopefully, a little less frustrated in the process when we come across these problems.
Dr. Adam Nally: Exactly.
Jennifer Marie: So, have a wonderful evening, everybody. We’ll see you later. Thanks for coming on, Dr. Nally.
Dr. Adam Nally: Thank you for having me.
Or you can watch it on our YouTube Channel here: