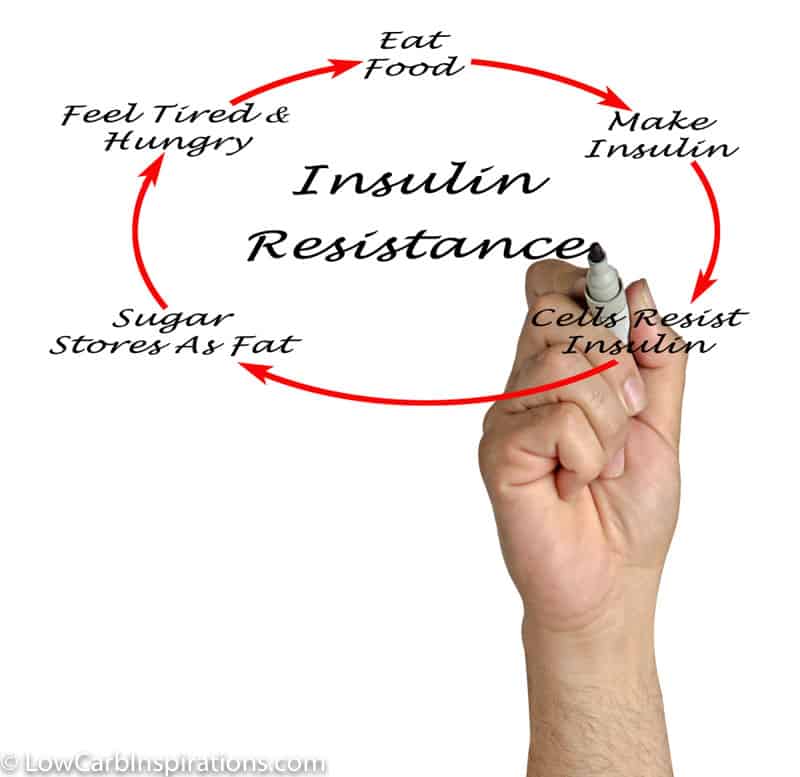
Insulin Resistance (What you need to know to fix it!)
I want to introduce you to an expert in Insulin Resistance! His name is Dr. Adam Nally! I had the pleasure of meeting him at KetoCon this year. I invited him to live stream a Facebook video with me to help my audience understand everything you would ever want to know about Insulin Resistance. The who, what, why, and how it came to be. This is some seriously interesting talk! Dr. Nally, aka DocMuscles, knows what he is talking about. Not only is he a Board Certified Family Physician and an Obesity Medicine Specialist! He runs an obesity clinic that has been in practice for 20 years! He’s seen it all!
Dr. Nally has done tons of research and tests because of his own struggles with obesity. This is why he has such a passion for the subject. I am a big supporter of anyone who puts this much effort into spreading the word of good health and nutrition!
You can head over to DocMuscles.com to find The Skinny on Sweeteners writeup he mentions in this interviews here. Be sure to sign up for his email once you’re there too. You won’t want to miss any information that he puts out! It’s really informative information that can help you on your own weight loss journey.
Dr. Nally is also a co-author with Jimmy Moore for the book he wrote titled The Keto Cure. I just ordered this book myself! I can’t wait to dive into it!
You can also find Dr. Nally on YouTube! Head over here to watch some of his past videos.
Watch the Insulin Resistance Interview with Dr. Nally here
Insulin Resistance Interview with Dr. Adam Nally Transcribed
Insulin Resistance – Why do we get it and how to fix it
Jennifer Marie: Hey, friends, we’re back. Guess what? Dr. Nally is in the house. Sorry about earlier. Sorry about the whole 7:00 thing. Dr. Nally and I attended KetoCon this weekend. It was exciting, amazing and exhausting all at the same time and, luckily, he came on very last minute. Dr. Boz will probably be back next week. Dr. Nally, the reason why I asked him to come on, first of all, he’s amazing, but second of all, I saw his YouTube channel at YouTube/drnally. He has an amazing video on, in fact, I think it’s a top video for you on insulin resistance. This is the topic we wanted to talk about this last week. Of course, as Dr. Boz and I ran out of … We talked and talked, we ran out of time and didn’t get to insulin resistance and it was on the list. You are a pro. I’ve told everybody already that you’re a board-certified family physician and you’re an obesity medicine specialist and you’ve been running a clinic for 15 years, I believe.
Dr. Adam Nally: 20 years actually.
Jennifer Marie: 20 years?! You definitely know what you’re talking about. I welcome you to this channel, the Keto friendly recipes page on Facebook. We’ve got so many people that are saying hello. Hi, everybody. Hi, John. Hi, Kathy. Hi, Christie. Thanks for tuning back in. Hey, Joe. Glad you could catch us. Let’s talk insulin resistance, the why, the how, the what, the what the heck?
Dr. Adam Nally: Let’s do. Do you want to start with a question or how do you want to start it?
Jennifer Marie: Well, you know what? Can you tell us? I think there’s a lot of people on here that really don’t even know, what the heck is it? We hear insulin resistance. We don’t I think even understand what it is. Maybe give us a basis of it. We want to know how to fix it. We want to know why we have it. We want to know what are the signs of it, just whatever you can tell us about this crazy thing that we supposedly have.
Dr. Adam Nally: The first section of my book is essentially about insulin resistance and it’s because what I started seeing in the first five years of my practice was this pattern, this pattern of people showing up with skin tags and thickening around the neck and weight gain that wouldn’t respond to caloric restriction and exercise. I had the same problem. My father had it. There’s a whole slew of reasons that it’s there. It’s not really a disease. I think it’s a response to our diet and our environment in a number of capacities, but specifically, it’s a response to our body’s intake of starches and carbohydrates and sugar. Some doctors blame it all on fructose. Others blame it on simple table sugar. In the 20 years that I’ve been in practice, I see it once you have this response that is abnormal, you respond this way to all starches and all carbohydrates. The approach to treating it is really trying to reverse that.
Dr. Adam Nally: To make it simple, 20 years before you ever become a type 2 diabetic, your body begins to overproduce insulin. I say it this way. If you were to give me … I’m insulin resistant. My father weighed 400 pounds before he passed away at 58 from all the complications of diabetes. His labs and my labs looked identical in our early 30s. If you give me a piece of bread or anyone a piece of bread, you should theoretically produce a slice worth of insulin from the pancreas to use and absorb the glucose and the fructose that’s in that breath or the sugars essentially. If you give that piece of bread to me, I literally produce 10 times the insulin response to that bread.
Dr. Adam Nally: Insulin stayed [negative 00:03:57] for 12 hours. If I eat a piece of bread for breakfast, I produce 10 times the insulin response for the next 12 hours, unless they have a piece of bread for dinner, I’m literally producing 10 times the insulin 24 hours a day, seven days a week. Insulin is the most powerful hormone in stimulating inflammation. It’s the most powerful hormone in stimulating changes in cholesterol. It’s the most powerful hormone stimulating your blood pressure. It literally drives the weight gain. It literally pushes the triglyceride and cholesterol into the fat cell. Without insulin, you will not gain fat. If you take the way the insulin from a type 1 diabetic, they are skinny as a rail. They cannot gain weight. Insulin is the only hormone that allows you to gain weight. If you’re gaining weight, you’re overproducing insulin, period, end of story.
Dr. Adam Nally: That’s what I see literally with 85% of the people in my practice and I have for years and years. I started studying very heavily, what is this insulin resistance thing? A guy named Joseph Kraft did 13,005-hour glucose and insulin tests a number of years ago. I started and I read his work.
Jennifer Marie: Is that orange drink of sugary-
Dr. Adam Nally: Just like when you have that drink they give you when you’re pregnant in that two-hour glucose tolerance test that every woman I’ve ever talked to hates, can’t stand it. It made them sick to their stomach.
Jennifer Marie: I passed out.
Dr. Adam Nally: Yeah, because people get hypoglycemic from it. Well, he did that to people, and he actually gave them five grams more than they normally do. He tested not for just two hours, but he tested glucose and insulin for five hours thereafter, and he recorded it. He saw what I’ve been seeing for years and years and years is that not only does the glucose spike and then bottom out and many people will get hypoglycemic, but the insulin level spikes up to 40 times higher than normal in some people, 40 times. That’s why some of us that walk by a bakery, we just walk by and we gain weight.
Jennifer Marie: Is that true? You smell the bread and you’re like [crosstalk 00:05:52].
Dr. Adam Nally: Literally, you smell the bread, there’s an insulin response.
Jennifer Marie: Yes.
Dr. Adam Nally: Literally, yes. There are people that have that challenge. I was one of them. My father was one of them. All of the Nally men, most of us, have this tremendous insulin resistance. I suspect this is a genetic protection because my family all comes from up in the Scandinavian countries where there was snow all the time, and we rarely saw carbs, and then all of a sudden, you introduced us to carbohydrates, and we go, woohoo, and we store fat for the next 365 days a year. It’s not really a disease as much as it is a syndrome of the inappropriate insulin response to a diet that literally is 85% sugar 365 days a year.
Jennifer Marie: Wow. That’s crazy. Christie said, “That’s real. I knew it.”
Dr. Adam Nally: It is real, Christie. It’s absolutely real, totally real.
Jennifer Marie: Wow. Hey, we have a couple of questions here if you’re ready unless you want to-
Dr. Adam Nally: I am ready.
Jennifer Marie: Kenny and Tammy says, “I was told I have insulin resistance and I am not a diabetic. Labs are perfect. A1C is 4.1. Cholesterol great. No response to keto diet or 96 hours of fasting. Any advice?” He’s probably going to give very general advice because we’re not allowed to give doctor-patient advice on this channel, but what would somebody do if they’re really struggling? They’ve done the keto diet and she’s not diabetic and her A1C is great.
Dr. Adam Nally: Remember, and this is the whole premise, I think on one of the videos, we talked about insulin resistance, I actually show you the graph. Insulin resistance is there 20 years before you ever qualify for a type 2 diabetic. That insulin level increases and increases and increases over time, so you may very well have normal hemoglobin A1C, the HbA1c number. You may have a normal fasting blood sugar, but you’re going to be gaining weight. That’s classic. If I were to do a two or three-hour insulin response test to you, your fasting insulin levels should be less than five. The lab says fasting insulin should be under 20. That’s wrong. It should be under five. Your two-hour recovery of insulin should actually drop to 40 within two hours. Most people are still at 100 at two hours.
Dr. Adam Nally: To be frank, the real true way to test, are you really insulin resistant, is to check your insulin at a fast and check your insulin two hours after a meal. Most people don’t want to do that because it’s a horrible test and it’s expensive. Most insurance, most docs don’t want to do it. Every time I send patients for that, the lab would say that Dr. Nally is crazy.
Dr. Adam Nally: The other way to do it is if you have skin tags, I guarantee you have insulin resistance. If you have little polyps in the skin anywhere on your neck and arms, that’s pathognomonic. Meaning it is the true one sign of insulin resistance.
Jennifer Marie: I had some, and I think two years into my journey, they started to fall off or lessen or lighten. Does it take that long to correct because [crosstalk 00:09:02] is asking. She said it can take 12 to 24 months to correct insulin resistance. Is that correct, Dr. Nally?
Dr. Adam Nally: That is correct. That is what I see clinically. It takes 18 to 24 months for people’s insulin resistance to begin to improve. That was one of the things that I’ve seen over and over for the last 15 years of doing this with myself and with my patients, is that it literally … The reason is this. It’s not a broken pancreas. It’s a broken fat cell. When the fat cells get bigger and bigger and bigger, the fat cells produce 178 normal hormones, 177 of which are all inflammatory. Eight of those hormones are what drive the liver to keep the blood sugar slightly elevated, and two of them damper down the effect of insulin on the liver. What’s happening is you have fat cells that are overproducing hormones that are making the excess insulin not work so the pancreas produces more. It takes about two years for the fat cells to shrink down and correct this abnormal hormone balance that’s occurring.
Jennifer Marie: Wow. Basically, you know you have it if you’re overweight, you have skin tags, the darkness on the back of your neck. Any other signs?
Dr. Adam Nally: If you’re a female and your waist circumference is greater than 35 inches around your waist, so that’s measured right at the top of the hip bones, just underneath the belly button, that’s the measurement. If it’s greater than 35 as a female, you’re more than likely you have insulin resistance. If you’re a male and it’s 40 inches, you probably have it. Most men will never come near a measuring tape. I just tell the guys, close your eyes and walk through the wall. If the first thing that touches the wall is your stomach, you have insulin resistance. That’s how guys figure it out.
Dr. Adam Nally: Skin tags, acanthosis nigricans is that darkening skin around the neck. Other classic signs would be if you have carb cravings every two hours, more than likely, and if your triglycerides are over 150, almost 95% of those people have insulin resistance.
Jennifer Marie: How do you fix it then? Is it just … I know you and I are very big promoters of the keto diet, high fat.
Dr. Adam Nally: The issue is there is no pill that fixes this. That’s the problem. The only way to fix it is to get the fat cell to begin to shrink. The only way to get the fat cell to begin to shrink is to stop pushing fat into the fat cell. Remember, the one hormone that drives fat into the fat cell is insulin. If insulin is on, it turns off the back door so the fat cell closes and it turns on the front door and fat enters. When insulin goes down, the front door closes and the back door opens up and fat exits, if that makes sense. It’s one of five back doors of the fat cell that lets fat out, is insulin. It has this push-pull effect on the front and back.
Dr. Adam Nally: We want to bring the insulin level down. Anything that’s going to raise your insulin level is going to propagate this insulin resistance. Anything that brings the insulin level back to a baseline … We don’t want to turn insulin off. Insulin is essential for both glucose metabolism. Insulin actually is essential for ketone metabolism, but we don’t want to turn it off. We just want to bring it back to a baseline. That takes literally restriction of starches and carbohydrates. Some people can see that with 100 grams of carbs or less. For people like me, we have to drop it all the way down to less than 20 grams per day.
Jennifer Marie: When you’re talking about this insulin test, and it’s hard to go to the doctor and you have to go get it done, most of this audience here has the glucose monitor along with the ketone. Is there a way we can be checking it with that?
Dr. Adam Nally: You have to extrapolate, and that’s the challenge, and that’s where the glucose ketone index has come up. That’s where all these different pieces have come up. Trying to find out, is there a way to bridge this without doing this really expensive insulin test? Unfortunately, as of yet, there’s not. To diagnose insulin resistance, if you have at any time in your life had a fasting blood sugar higher than 99, and in my office higher than 95 is my cutoff, then you have insulin resistance. If at any time you’ve had any blood sugar randomly two hours after a meal greater than 140, you have insulin resistance. If you check your blood sugar and it’s 142 and it was two hours since your last meal, you’re insulin resistant. If you wake up first thing in the morning and you check your blood sugar and it’s 101, you have insulin resistance.
Jennifer Marie: That explains, I’ve been doing this a lot longer than my husband. He wakes up with higher blood sugars, and I don’t. I’ve been doing it so long, I never tested my blood in the morning. I was hypoglycemic. I’ve done very well on the keto diet. Now when I test my numbers, I’ve got really good sugars like in the 70s, and when I fast, I can get down. I can those ketones up and get those sugars down and be in a really good ratio. My husband, he’s like, “I’ve been doing this. What’s wrong?” He’s under a year doing it and he’s like, “Why do I wake up with 199, 101? This is not right.”
Dr. Adam Nally: He’s still insulin resistant. I’ve been doing this for 15 years, and if I cheat, I will literally see morning sugars of 102, 107 still to this day. It’s related to a small amount of fat that I still retain around my belly, and it’s genetic and it’s slowly shrinking, but it’s taking me time. My practice is significant … My average patient age in my office is 65 or older, so I have a very heavy geriatric population in my practice. I work out in the Sun City here in Arizona. A large percentage of my patients are over 65 that are Medicare age. One of the challenges that I found was a lot of them couldn’t exercise. I don’t usually do anything unless I experiment on myself first with my patients.
Dr. Adam Nally: With this, because there was not a lot of data about it, I started doing it, and I stopped exercising. Other than throwing hay out to my horses every weekend, I used to run triathlons and all sorts of stuff like that. I stopped doing that for about 10 years, and I just followed a diet, and I lost 65 pounds, and I maintained it. That little last bit of fat around my belly I could not get rid of until I started reinstituting exercise, specifically resistance exercise and running. In the last year, I’ve dropped another 15 pounds, and it’s still coming off little by little, but that insulin resistance still hangs on, and it does so because of, one, genetics and, two, various sweeteners and things like that play a role there too, but there’s a whole slew of reasons, which is probably a whole other podcast in and of itself. Go ahead.
Jennifer Marie: We talked about the higher blood sugars in the morning, but what about that dawn phenomenon? Because that’s what everybody is saying that when you start waking up and the cortisol. How does that play a role?
Dr. Adam Nally: If you’re insulin resistant, what happens is, especially this happens especially with diabetics but even those that are insulin resistant will see this happen. If you eat a meal that’s higher in starch or sugar the night before, what happens is your body overproduces insulin. Remember, that insulin lasts for about 12 hours in your system. It’s most active in the first two to four hours, but it’s still present for 12 hours. If my dinner was four Krispy Kremes, a Ding Dong and a Twinkie, then what would happen is my blood sugar would spike quite high and I would feel fine. I would go to bed and that blood sugar would go way up, and my pancreas would go, holy cow, and it would shoot a bunch of insulin out.
Dr. Adam Nally: By about 3:00 in the morning, my blood sugar would bottom out and I’d get hypoglycemic. I might wake up. I might not. You don’t know how low it goes, but then the liver goes, wow, and the liver then dumps out a bunch of glucose into your bloodstream. Within about a three to four-hour window, all of a sudden, your blood sugar jumps up to 110, 120, and it’s called the dawn phenomenon. It’s a response to a spike in insulin. You can get that from a meal. You can also get that if you’re a type 1 diabetic and you overshoot your insulin. That’s another way that it can happen. That’s what the dawn phenomenon is.
Jennifer Marie: If you guys are finding this insulin resistant talk helpful, if you can share this out, I feel like this is such good information that not many people are talking about and hit the share button. I also want to mention that, I know I said it earlier, but we have so many more people that have jumped on since we started. You can find Dr. Nally at docmuscles.com. You can find him on youtube/drnally. Can you tell them about your Instagram?
Dr. Adam Nally: Instagram is @docmuscles. If you type in docmuscles on Google, it’ll pop up a bunch of stuff too. That’s D-O-C-M-U-S-C-L-E-S, DocMuscles.
Jennifer Marie: We have a lot of people asking about menopause and insulin resistance, which I think they’re at my level, totally deep in menopause.
Dr. Adam Nally: The really cool thing that I find … That’s not cool because it causes problems and people think they’re dying from it. I’ll start someone on a ketogenic diet and they’re in their perimenopause or menopause region. One of the things we have to remember is that estrogen and progesterone and testosterone are all bound with fat. That’s how they function, especially estrogen. If you carry extra weight, what happens is that that estrogen gets get stored into the fat cell with your fat molecules. As you start mobilizing more fat and that fat is released out of the fat cell, all of a sudden your estrogen level goes up. Well, if you’re a female, and you know what happens when progesterone goes down and estrogen goes up, you have a cycle or you have hot flashes or you have a period and a flux, and they’ll do that for two or three months with a lot of patients.
Dr. Adam Nally: I have patients that will have great fat loss then they cheat and they go off for a while, and then all of a sudden, they start having hot flashes. They said, I thought I was passed this hot flash issue. Well, what’s happening is you’re now mobilizing estrogen and hot flashes occur or the menopause symptoms occur when estrogen goes up or estrogen goes down. When estrogen is stable, you don’t feel those symptoms. When progesterone and estrogen are balanced, you’re less likely to have the hot flashes that occur, but it’s the flux of estrogen up or down the drives the hot flash. Initially, I tell women, don’t be surprised. You’re going to have hot flashes. You’re going to feel weird for the first month or two. That’s normal, but it should level off, as long as your fat loss is staying consistent.
Dr. Adam Nally: If you’re cheating, if you’re doing things that are sabotaging that progress, you may see that fluctuate. If you don’t see it resolved within two or three months, then we want to truly look at your female hormones or your male hormones if you’re male and say, where are they at? Do we need to fix it? A predominant number of my patients are estrogen dominant, meaning because of a whole number of reasons, it’s not the estrogen level or the progesterone level per se. It’s the ratio of the two together that really makes people feel good or bad.
Dr. Adam Nally: What happens is a large percentage of things that we eat, a large percentage of our cosmetics actually stimulate estrogen-like responses. We have a lot of women that are symptomatic estrogen dominant. Even though progesterone, when you were pregnant caused you to restore extra fat, too much estrogen, will also cause you to store fat, especially around your hips. If you have that pear shape, guess what? You’re estrogen dominant.
Jennifer Marie: That’s totally me. Oh my, god. It’s funny because I did really well on keto for two years. I had some hot flashes when I first started, and that was the movement of exactly what you’re saying, the estrogen in the fat cells. It happened again. I had stayed really, really strict, like really strict for two years. All when that was happening, I was very, very strict. I noticed that when I really started fasting or pushing or stressing my body to lose more, that’s when the hot flashes would go up. They were hard and heavy and it was horrible.
Dr. Adam Nally: You’re mobilizing fat and releasing more estrogen is what happens with that frequently. The second issue is if you’re on a synthetic form of estrogen and/or progesterone, the synthetic form of progesterone will not cross the blood-brain barrier. It works from the bottom half of your body down, but it doesn’t work from the top half. The challenge is that part of that modulation of the ratio if progesterone can’t cross the blood-brain barrier and the estrogen can’t do so effectively, then you’ll also have hot flashes. One of the reasons I’m a big proponent of bioidentical hormones is because we want that progesterone to be able to cross that blood-brain barrier and all of the synthetics don’t. That’s one of the big challenges with the synthetics.
Dr. Adam Nally: In medical school, all of us were taught use Premarin and use these forms of estrogen, but they’re all synthetic, and that caused a whole slew of other problems that a lot of women have suffered with as well. If you’re not seeing success with where you’re at with your hormones, you need to have your doctor check. You may consider using the bioidenticals because for my patients, that’s been a huge change for them.
Jennifer Marie: Wow. I know that the scale has stagnated, which is fine. I haven’t gained, which is great. The hot flashes are gone, thank God. I’ve wondered. I am on synthetic, and I’ve been told you really need to look at this, and now I’m scared to change for fear of messing things up.
Dr. Adam Nally: If you change, you want to do so really slowly. The challenge that I have with most patients is that they want to just fix it overnight, and it takes literally 60 days to balance progesterone. It takes 90 days to balance estrogen. You’re looking at three to six-month process of fluctuation, and it’s a slow process and you just have to be prepared for that and say, okay, I’m ready to do it. Remember, estrogen and testosterone are two of the back doors of the fat cell. If your estrogen levels are too high and testosterone is too low, you will not see that weight move, and that’s one of the reasons for plateau frequently for a lot of my patients.
Jennifer Marie: We’ve got a lot of questions. Cynthia Armstrong says, “This explains so much.” It does, doesn’t it? I love the way you explain it. It’s so easy to understand. Let me look at the comments. Teresa says, “I have a lot of skin tags. I’ve been keto for six months, only lost 19 pounds.” What do you mean only? That’s terrific. That’s wonderful. “My hormones are out of whack.” Girl, he just explained why. That makes sense.
Dr. Adam Nally: Let me interject something for your wonderful audience, and I have to explain this over and over to patients. I have to remind myself of it. The scale lies. I tell people, take the scale and give it to the neighbor you don’t like. All I want you to do is follow your waist circumference. That’s what I want you to do. If your waist is shrinking, you’re seeing success. This seems to be more predominant with women than it is with men because, number one, men really don’t get on a scale. Number two, they see their waist move fairly quickly because they have testosterone. Women have a lower level of testosterone so it doesn’t move as fast.
Dr. Adam Nally: If I take a cup of muscle and a cup of fat, that cup of muscle, the volume of muscle literally weighs twice as much as fat. Many women who have excess body fat cannot make muscle. As soon as you now allow the body to start making muscle, even without exercise, if I give you the right diet, your body will say I got to put more muscle on, and it will do so. The scale weight may not move, but your waist will shrink.
Dr. Adam Nally: The mantra in my office is “stop getting on the scale.” Let your doctor measure you once a month and they can make your pants fall off. That’s the rule of thumb. If you’re seeing your waist shrink, you know you’re seeing success. Don’t worry about the scale.
Jennifer Marie: Good. Mary says, “That darkening of the skin, can that happen on your knees and your elbows too?”
Dr. Adam Nally: Absolutely. Around the neck, under the arms and the elbows and the knees, behind the knees, even on the tops of the feet. I’ve seen it behind the ears in some people.
Jennifer Marie: Wow. Somebody says they’re going to have to read. Christie says, “I’m going to have to rewatch this for sure.” Definitely, right? Dr. Nally talks really fast so I’m going to watch it-
Dr. Adam Nally: I talk really fast. Yeah, I get excited and I talk really fast. If you need me to slow down and repeat, please tell me, because I get so excited about this stuff. My wife says slow down, Adam. Stop it.
Jennifer Marie: I’ll tell you what I’ll do. I will have this transcribed, and I will put it in a blog post because this is so important. People really want to hear it. They want to know what’s going on. They want to know why, how, what and how can we fix it.
Dr. Adam Nally: Exactly.
Jennifer Marie: Let me go back. Thank you guys for sharing that. There’s a lot of people that said they shared, so thank you so much for that. We are definitely here. We do this to help people. If you can share it, that helps people. Christie says, “It’s like type 2 diabetes. Once you have it, you have it. It can be helped but it doesn’t go away if you stop taking care of it.” I would say yeah, that’s correct.
Dr. Adam Nally: It takes time. Remember, you didn’t get here overnight and you won’t get there overnight either. It takes time, years we’re talking. It’s a slow process, little by little. I just have to keep reminding patients. I have to remind myself as well, this is a slow process. What’s really cool is that metabolically, you’re going to be metabolically healthy before you see the weight come off completely. That’s the most healthy way to be.
Jennifer Marie: How do you know you’re metabolically healthy?
Dr. Adam Nally: For instance, in my 30s when I was in medical school and eating really healthy hospital food in residency, my triglycerides were over 400. My A1C was at 5.6, which is literally almost diabetic. I was 65 pounds heavier than I am today. My blood pressure was in the 160s and 170s. In fact, every time they took my blood pressure, they wanted to send me to the ER. I was the ER resident. I was a walking time bomb and I felt great, but I was a walking time bomb just like my father. My father ended up, he literally weighed 400 pounds. At 42, he had a quintuple bypass, which is five blood vessels. Three years later, three of those had to get stented. Actually, five years later. Then he went into renal failure. He was on dialysis. He had what’s called Charcot joints of the feet, which means the heels collapsed and he couldn’t walk. Every complication of diabetes, he had it. My labs and his labs look identical.
Dr. Adam Nally: Today, I’ve been doing this now for 15 years. I’ve been living this lifestyle for 15 years. My A1C is now from 4.9 to 5.0. My triglycerides dropped from over 450 down to the last check was 51. My blood pressure is always under 110 now. I’ve literally maintained my weight where I’m at right now, 15 pounds lighter for over 10 to 12 years with very minimal exercise. My job is high stress. I work 12 to 18 hours a day in the office and I’m home charting. Being a physician is high stress, and I’ve been able to maintain weight with that high cortisol that’s always there. All of my patients are the same way. We see that same profile change literally within a couple of months. The weight comes down afterward, but you have to be metabolically healthy before you start seeing that weight come off.
Jennifer Marie: If you guys want to see a picture of him, I took a picture with him at KetoCon, and you can find it on the Instagram page for Keto friendly recipes. Go over and check it out. You can see exactly what he looks like. He’s a big bulky guy, and I look like a little person next to him. Cathy is asking, “What are your thoughts on artificial sweeteners?”
Dr. Adam Nally: I have lots of thoughts on artificial sweeteners, Cathy. In fact, I wrote a whole chapter in the book. You can actually get that. That chapter is on my website at docmuscles.com. Go to the menu and click on freebies and it’ll talk about the skinny on sweeteners. The entire chapter is right there. Sweeteners have been the bane of my existence. There are only four sweeteners that I’m comfortable with that don’t raise insulin. One of those still stimulates insulin resistance in the gut bacteria and so it can be a problem so we have to be careful with it. I’ve written out all of them.
Dr. Adam Nally: I’m okay with erythritol. I’m okay with Liquid Stevia. I’m okay with chicory root. In my practice, I’ve used aspartame because as obesity docs, we were taught to use that because it suppresses the appetite and it doesn’t stimulate the insulin response. Aspartame does bother the gut bacteria and can propagate insulin resistance in the gut. I will often bridge people with the use of aspartame and then try to get them off later. Those are the only three that I ever recommend.
Dr. Adam Nally: Any of the other sugar alcohols you want to avoid like the [pleg 00:30:03], especially acesulfame potassium, which is the most commonly used sweetener currently in most of the diet or low carb foods. You have to be very careful with that.
Jennifer Marie: Which one is that, a brand name?
Dr. Adam Nally: Acesulfame potassium. It’s not sold in the … You can’t cook with it, but it’s in most soft drinks or most low carb drinks or most low carb bars and shakes. The one that I see a ton of use now with a lot of low carb products, and the low carb people are going to hate me for this, is monk fruit. About 50% of my patients will actually spike insulin. I’m one of them. It will spike insulin with the use of monk fruit. Monk fruit is a fructose.
Jennifer Marie: I’ve read that. I’ve read that there are some people that are highly sensitive to monk fruit and some-
Dr. Adam Nally: I’m one of them. Yeah.
Jennifer Marie: Some people it doesn’t. I love monk fruit and I’ve tested my glucose. It has not done anything to me.
Dr. Adam Nally: Remember, 100% of fructose is metabolized in the liver, and fructose and alcohol are metabolized identically. What happens is it enters the liver. It’s changed into an aldehyde. That aldehyde then produces an insulin response five hours later. You won’t see the insulin rise from fructose or monk fruit for five hours. For me, it stimulates cravings two hours later because the aldehyde stimulates the same aldehyde that morphine does in the brain and goes, whoa, that was really good. Two hours later, you want a donut. That’s the challenge.
Jennifer Marie: You said liquid. I heard you say specifically liquid.
Dr. Adam Nally: Liquid Stevia. I actually grow Stevia in my garden. Stevia is a plant. To get the Stevia out of it, you actually have to press the leaf, and it’s a liquid. To make it a crystal, they bind it to something called dextrose or maltodextrin. Those are just two forms of sugar that work for the FBI or the CIA and so you want to be cautious because when Stevia is in a crystalline form, it’s usually down to a form of a sugar. That is the form of that sugar that’s the problem, not the Stevia itself.
Jennifer Marie: Wow. Catherine wants to know, do you manage any patients via telemedicine?
Dr. Adam Nally: I do what’s called … I have a concierge service, but the challenge because of Arizona medical law is I have to actually physically see you face to face at least once in my office in Arizona. Once I’ve established a relationship with you in Arizona face to face in my office, then I can treat you via telemedicine in various places. Some states have various laws, and so we have to be cautious with those, but for the most part, I can treat you because we’ve established care face to face. The challenge is that I’m looking into doing some specific nutritional counseling, but my medical law basically says that still falls under the practice of medicine so I have to be real careful with that. I have patients that do come out of the direct primary care in Arizona. I have patients that come to see me from all around the world, but they have to see me at least once a year in my office face to face, and then I can do telemedicine outside of that.
Jennifer Marie: Cathy Parsons Crawford is saying, “You have to come back again.” She is loving this. Well, guess what, Cathy? Doc Muscles and I … Do you mind if I call you Doc Muscles?
Dr. Adam Nally: That’s fine. Yeah. Adam, Dr. Nally, hey you, I respond to all that.
Jennifer Marie: We talked at KetoCon. We talked before this. We are definitely going to do something again and again and again because this is too much fun. It’s a lot of information. It’s really good information that I think people need. You know what? There’s a lot of people … I think the guys would probably want us to talk about testosterone because I’m certain that the same thing that you’re talking about with the cells and everything has an effect to guys’ testosterone too, right?
Dr. Adam Nally: Oh absolutely. I actually did a presentation at the Metabolic Health Summit in Los Angeles in January on testosterone. Testosterone is one of my favorite things to talk about. 60% of the men that come to me in my office that are insulin resistant have low testosterone. It drives a whole problem, a whole slew of men’s issues. Yes, that’s a huge topic that-
Jennifer Marie: My husband would want to talk to you, for sure. He gets shots, and he’s been doing the diet. He’s down 85 pounds.
Dr. Adam Nally: Oh, that’s awesome.
Jennifer Marie: Oh, amazing. He’s always carried his weight in his stomach and he’s given up beer, which that is a miracle in itself. I didn’t think he would ever do it, but he did. He’s like a total rock star. I think we definitely … Testosterone is probably a whole another talk, isn’t it?
Dr. Adam Nally: We could talk for two hours about testosterone. I’ve actually done it. If people want to know right away, if they go to my YouTube channel, they can actually see. I’ve done two different, a short and a longer presentation on testosterone for my YouTube channel. There’s some stuff there already. I’d say that would be a great thing to talk about for your audience.
Jennifer Marie: Good. When I write out this blog post, I will link that testosterone video in the blog post also so people can find it. Gale wants to know, do most of your patients fast also? Are you big into fasting?
Dr. Adam Nally: The literature right now, let me back up and quantify. The ketogenic diet, if it’s done correctly, stimulates natural periods of fasting. I normally don’t eat breakfast because if I eat a good meal at dinner, I’m usually not hungry until 12:00 or 1:00. I don’t normally eat a meal in the morning. My first meal is at lunch and then I’ll have dinner. Usually, I do two meals a day.
Dr. Adam Nally: When I first started doing this because I was so insulin resistant, I was ravenous. I literally ate a pound of sausage and three eggs cooked in butter every morning for almost two or three months, then I would have a double burger wrapped in lettuce at lunch, and then I have a big piece of meat with a salad at dinner. I did that for a few months. All of a sudden as I became less and less insulin resistant, all of a sudden, my appetite suddenly went … I realized I could back that way down. I was eating about 5,000 calories a day for the first few months that I did this, and I still lost 65 pounds. That plateaus once you keto adapt around two or three months. That’s where a lot of people plateau because they still keep thinking they need to eat that much. They don’t.
Dr. Adam Nally: If you’re listening to your body’s hormones, which is the other piece that we talk about a lot, is I want you to start listening. When you’re full, stop eating. Don’t eat. Are you eating because you’re truly hungry? Are you eating because you’re bored? Are you eating because you’re stressed? I’d say check those reasons, and that’s usually why I …
Dr. Adam Nally: We go on the fasting question. I’m a big fan of intermittent fasting when you’re listening to your body that way. There’s argument back and forth right now with a lot of the fasting people. My big concern is that when I see people fast frequently for longer than three days, it dramatically suppresses testosterone by up to 50%, and it dramatically lowers the thyroid function permanently. I’m not a big fan of the long, prolonged fast, longer than three days. Once in a while if you did it, it’s not a big deal. If you’re doing it routinely, which I hear a lot of people doing, you can, at least according to the literature I’ve read in the two most recent studies, permanently suppress that thyroid function. That’s a big factor for a lot of my patients because they’re already behind the eight ball when it comes to the conversion of T4 to T3.
Jennifer Marie: wow. For those of you asking about The Keto Cure book, I went ahead and linked it in the comments. In the blog post, I will often put the link to the book. I just ordered it myself. I can’t wait to read it. I know Jimmy Moore as well. I’m a big fan of Jimmy. He’s a wonderful guy. Good. Wow. This is amazing, amazing information. I think we covered most of it though. Do you have anything else on insulin resistance that you had wanted to add or talk about?
Dr. Adam Nally: I saw somebody asked a question about they had lost weight but they still hadn’t lost weight around the chest or the breast. Unfortunately, the breasts are the last to go, the abdomen and the breast. The reason is that your body thinks even into your 50s and 60s that you may still want to have children and breastfeed. It will preserve that fatty tissue until the very last. For a lot of people, that will be the last thing to go.
Jennifer Marie: Interesting. That’s very interesting. Good to know. Let’s see here. Do we have anything else? Jamie says, “I just read The Keto Cure last month. Awesome content. Don’t wait to get it.”
Dr. Adam Nally: Thank you, Jamie.
Jennifer Marie: That is awesome. Look, I’m going to put it up there. Look. Thanks for that, Jamie. Selma says, “Excellent talk. Thank you.” You’re very welcome. If you guys want us, we’re going to try and brainstorm some topics and I’m really, really, really focusing on what is much needed and not given in the community. I know that insulin resistance was a big topic. If you guys have other talk topics that you want us to discuss or maybe schedule some future shows with Dr. Nally, put them in the comments if you don’t mind, and we can definitely go back and look at that and we can schedule. We’re hoping to do something weekly. I will still … Dr. Boz is definitely still going to be on. We love her. We’re trying to bring more experts on to the channel just to help everybody else who needs it. Thanks for tuning in, everybody. I’m not sure when our schedules will connect, Dr. Nally, but we’ll figure something out and we’ll announce it soon.
Dr. Adam Nally: Absolutely.
Jennifer Marie: All right. Have a good evening, everybody. Have a good night.
Dr. Adam Nally: Good night.


Great information !!
This was a great talk with so much information. I am continually shocked at how little the medical community in general knows and understands about diabetics and insulin resistance. My husband was in the hospital with what was originally diagnosed as a heart attack. He is also diabetic. Upon admittance he was taken off all of his oral diabetes medication and put on insulin. I thought they were surely going to kill him as they increased the insulin in response to increased glucose levels while feeding him a high carb diet. When his glucose levels reached 400+ we asked them to take him off insulin, explaining he was insulin resistant, resumed his oral meds, and hand picked food item from the menu. His glucose levels returned to normal. His diagnosis was changed to A-fib, for which he was treated without success. A year later it was determined that he had atrial flutter and was treated with a pacemaker, which has been successful.
Thank you for sharing this information. Can’t wait to read Dr. Nally’s book.
Thank you Jennifer and Dr. Nally!
Excellent video ! really learned a whole lot on insulin resistance.
Which is the group that I fall into, that I didn’t know I was .
Please keep the informative videos coming!
This was great Jennifer. Thank you.
Already a fan of Dr Boz and Jennifer Marie. Now I’m a fan of Dr. Nally! Great info! Thanks so much.